
You're Sick Because You're Flat
I'm manifesto-ing on circadian amplitude again

To my enormous chagrin, circadian rhythms are maybe like the fifth most famous biological rhythm. I’m putting them behind breathing, walking, and menstrual cycles, here—don’t break my heart by telling me they should be even further down.
But I’m grateful to the #1 most famous rhythm (heart rate) because it makes the point I want to make today very neatly for me: When your heart rate goes flat, that’s about as bad as it gets, health-wise. When your circadian amplitude goes flat: bad too.
No, you don’t instantly die. Flattened circadian rhythms are all around us these days, sagging under the weight of aging and disease or squished underfoot by our jobs and behaviors. That people can work nights, eat around the clock, and live with dementia for decades shows that this isn’t an instantly fatal prognosis.
It does eventually get you, though. And what’s unique about the way in which it gets you is that it almost never takes the blame. Death, asphyxiation, paralysis, menopause: when other biological rhythms go flat, we give it a name. You could tell me, for any one of those terms in the last sentence, exactly which rhythm has been lost.
Circadian amplitude suppression, on the other hand… Well, insomnia, ADHD, idiopathic infertility, chronic inflammation, and non-dipping blood pressure come to mind.
You seem to have skipped a lot of steps there, Olivia
This is fair. After all, we don’t really have a gold standard way of quantifying circadian amplitude in the first place. It’s awfully bold to suggest that the root cause of the conditions above and many more is “thing we can’t easily measure or define; just trust me.”
But being bold is what you get to do in blog posts. And in that spirit, I will now lay out my case for 1) what circadian amplitude is, 2) why it’s the best framework for capturing the idea of “clock bad,” 3) how we, in modern life, chronically suppress circadian amplitude through our choices and actions, and 4) what we need to prove all this is right.
What circadian amplitude is.
Well, you know (waves hands). It’s when a rhythm that used to look like this:
starts looking like this:
When I talk about circadian rhythms having “terrible UI” (that is, having a bad user interface as a concept for people learning about them for the first time) I usually mention the fact that there are so many circadian rhythms, which is overwhelming, which causes people to short-circuit and fall back on the much more mentally tractable “circadian rhythms = sleep.” If you, exposed to the prior sentence, are starting to affix a framed version of it to the walls of your mind, please imagine me spiking it out of your hands.
Yet amplitude also suffers from this problem. There are so many ways I could define it that it’s hard to have a coherent conversation about it, which means we just mostly don’t talk about it at all. But let’s give it a go while we’re here.
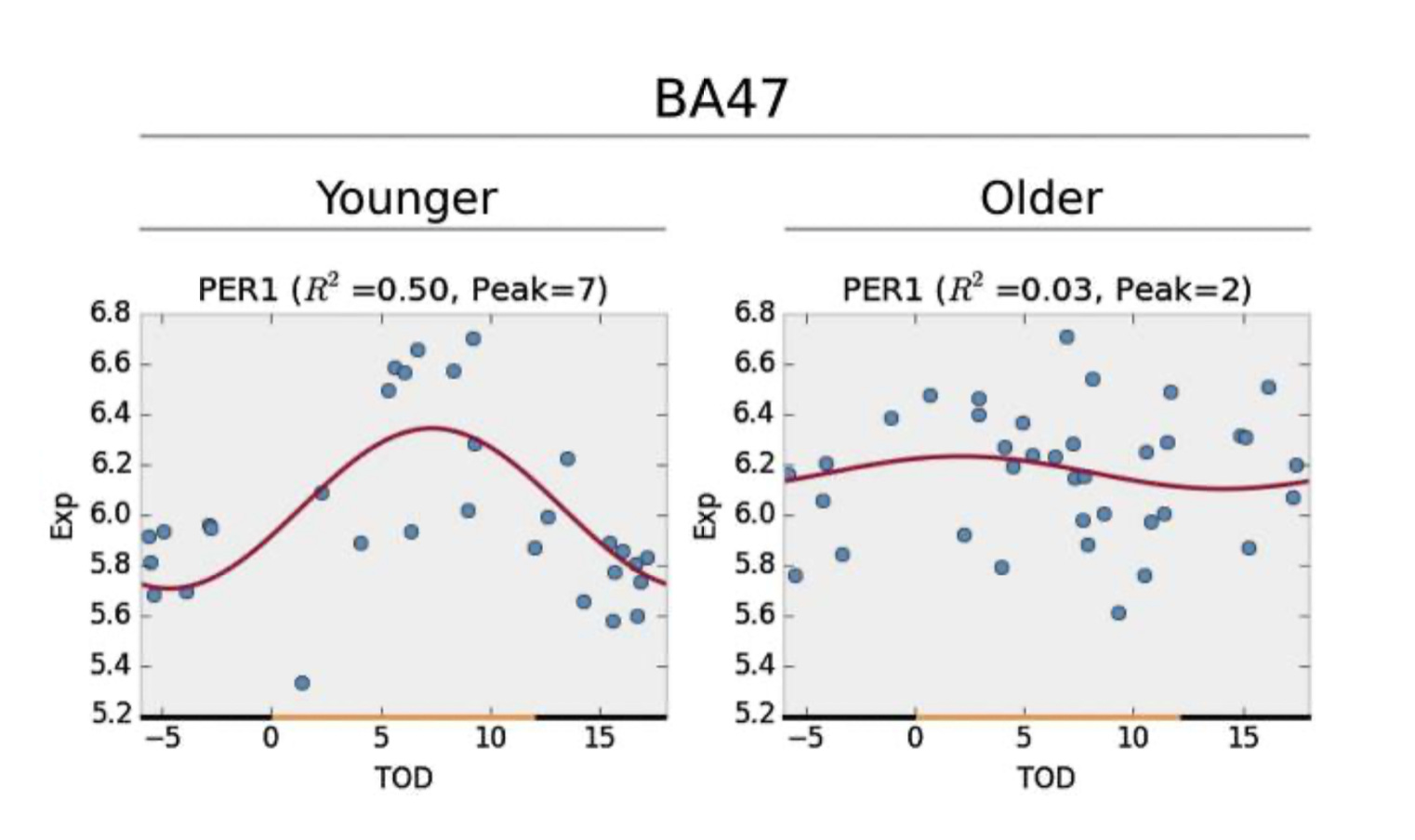
I could define circadian amplitude with any subset of the roughly 50% of the genome that’s rhythmic. Example: PER1 rhythms in this cell are blunted—they go up and down less than they normally do in healthy people—therefore you have low amplitude.
I could define it at the tissue/organ/whole body level in the same way, with behaviors dampened by gene or protein rhythms being low amplitude. But I could also define it at those scales as arising from high amplitude constituent parts that are out-of-sync with each other.
Think: teens jumping up and down together in an elevator trying to break it. If they’re in sync, their combined force causes the elevator to lurch and stall out and everybody screams and they get a good TikTok out of it. If they’re jumping out-of-sync, nothing happens. Now swap in “neurons in the suprachiasmatic nucleus” for “teens” and “breaking the elevator” for “sending an unambiguous day/night signal to the body.” That’s amplitude.

Finally, I could define a functional “utilization” amplitude, along the lines of “you need Process X at these times, but you have it at these other times.” Like this:
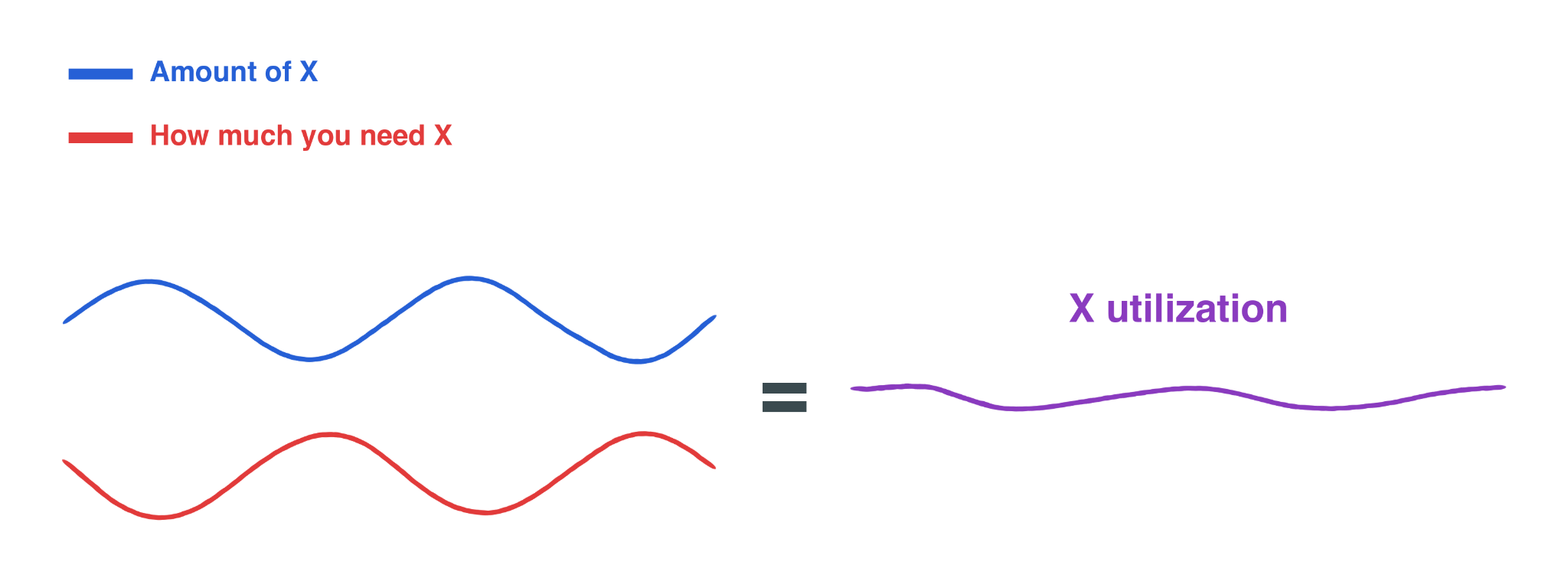
Your utilization is flat. This, too, is low amplitude.
Fundamentally, amplitude is confidence. Amplitude is the clarity of the day-night signal; the body’s certainty that its estimate of time is correct. High amplitude means your body can take more risks, get more gain. Low amplitude is a state of chronic uncertainty—a wobbling bike, a sputtering motor. A refusal to take the plunge and say with full-throated conviction “yes, THIS is the time for peak insulin sensitivity!”
Measuring anything resembling amplitude is a nightmare.
Say I want to try to estimate whole-body circadian amplitude using temperature.
It needs to be core body temperature to be a true circadian marker, which means you’re swallowing a thermometer pill or inserting a rectal thermometer; plus, we have to make sure you don’t sleep or move too much to avoid losing the circadian signal under the masking effects of sleep and motion. Plus we need to get the full 24 hours to make sure we’re seeing the full up-and-down of the rhythm over the course of the day.
Enjoy lying awake in the dark for 24 hours!
Even a full day of data collection might not be enough. Say I want to estimate your amplitude by taking the area under the curve of your melatonin rhythm. Once again, I forbid you from moving too much or sleeping. Once again, I take samples (spit, probably) from you over hours and hours to get a plot that looks like this:
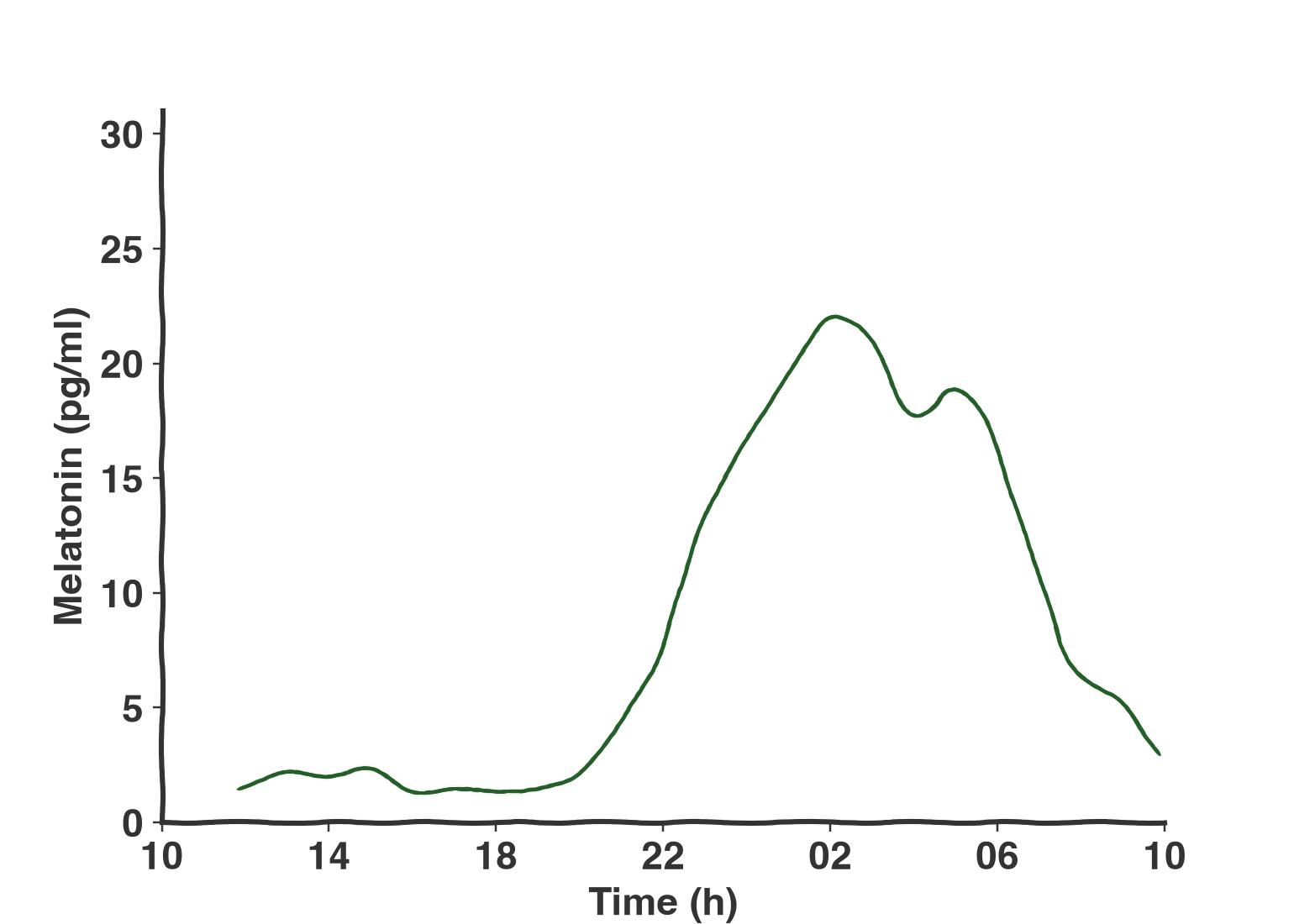
Except some people are just really high melatonin producers, for reasons that probably don’t have much to do with their circadian clock. Or, in other words:

Which means we can’t really use the entire day’s worth of melatonin we sampled to say something generalizable about their circadian amplitude. We can say things about changes within the individual, like “your melatonin amplitude is 20% higher than it was 7 days ago, the last time I made you sit in the dark for a full day as I collected your spit.” But what we want is a simple, one-off test that can say “hey, your amplitude is low,” and we don’t have that yet.
What we often default to is using “amount of daily activity measured from a wearable” as our definition of “circadian rest-activity rhythm amplitude.” Which, okay, I’m not going to say there’s nothing there, but there are certainly many more things driving what we see (movement) than what’s going on in the circadian part of your brain. Or:
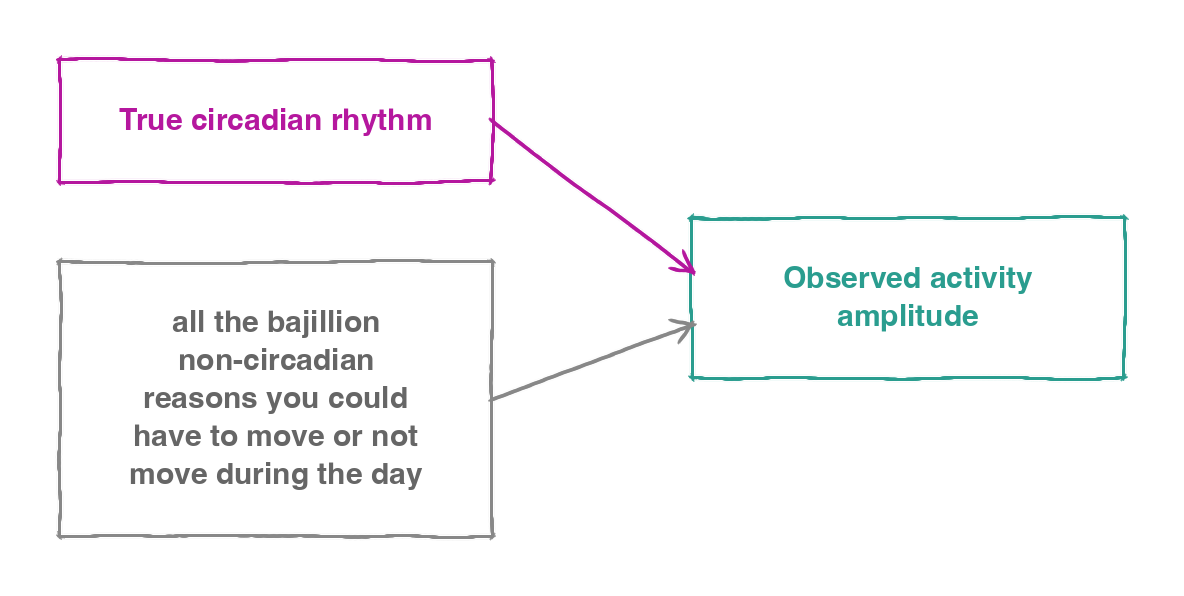
A shift worker could run a marathon one day and be categorized as high amplitude. A perfectly healthy person could be stuck in meetings all day and read as low amplitude. I could kidnap you and put you in a Saw-style trap where your arm is attached to a moving windshield wiper all day, until you agree with me that what we’re measuring is not a good representation of your body’s confidence of day-versus-night. During the time your arm is moving? Under a “did you move a lot” definition of amplitude, you’d look incredible.
So amplitude has no one definition, means different things at different scales, and is practically impossible to accurately measure with current tools.
Why circadian amplitude suppression is still the right way to talk about diseases of the circadian clock.
Plenty of terms out there are aimed at capturing the idea that you’ve screwed up your circadian system. Circadian misalignment, chronic jet lag, circadian disruption—these all imply some form of circadian injury. What drives me crazy, though, is that none of them go the extra step of spelling out why that injury is bad. There’s a gap where mechanism should be.
Amplitude neatly solves this problem. If rhythms are flat, then there is either not enough of something when you want it or too much of something when you don’t, both of which are bad.
Why is chronic jet lag bad? Because it squishes your rhythms.
Why is circadian misalignment bad? Because if you are forced to wake up or get light or eat at a time your body isn’t anticipating, it squishes your rhythms.
Why is circadian disruption bad? It’s not because you’re knocking your clocks into a healthier, more robust state. It’s because somewhere there’s a rhythm, and it’s flatter now than it was before you messed with it.
My claim: Behind every circadian problem there is, somewhere, a low amplitude.
Contrapositive: If you don’t have reduced amplitude somewhere, you don’t have a circadian problem.
Consider, for a moment, the person who is a night owl but a very happy, consistent night owl—who goes to bed and gets up at the same time every day, gets plenty of light during their waking hours through sun exposure and full spectrum artificial lighting, who has extremely dark blackout curtains during their rest periods, and who never has to get up early for work or school. This person might be flagged for circadian misalignment simply by virtue of being a night owl, but do they actually have a circadian problem? No! But if you made them start waking up at 5:00 am, the light and activity hitting their system at that time would blunt their rhythms.
{kind=link}
Consider next the person who has the most middle-of-the-bell-curve chronotype you can imagine; who keeps their wake-up and bed times precise down to the minute, but whose days are very dim (works in a basement) and whose nights are very bright (light pollution from outside). Does this person have a misalignment problem? Nope, nor do they have chronic jet lag or circadian disruption. But their amplitude is surely lower by virtue of the fact that they have massively reduced the contrast of the day-night signal to their brain.
And of course we can construct the example of a rhythm that is full amplitude, just horizontally shifted relative to where it’s needed, and all of the problems this person has in their life stem from the fact that this rhythm—appearing full amplitude to any passerby!—is not where it needs to be. But this is just my low “utilization” amplitude from above! Misalignment is low amplitude.
Uh, excuse me, what about gain-of-rhythmicity?
(Rusty geezer voice) Well, well, well. I thought you might bring up gain-of-rhythmicity.
A fun fact about aging and circadian rhythms is that you don’t just see existing rhythms flatten out as you get older. You also see previously flattened rhythms start oscillating.
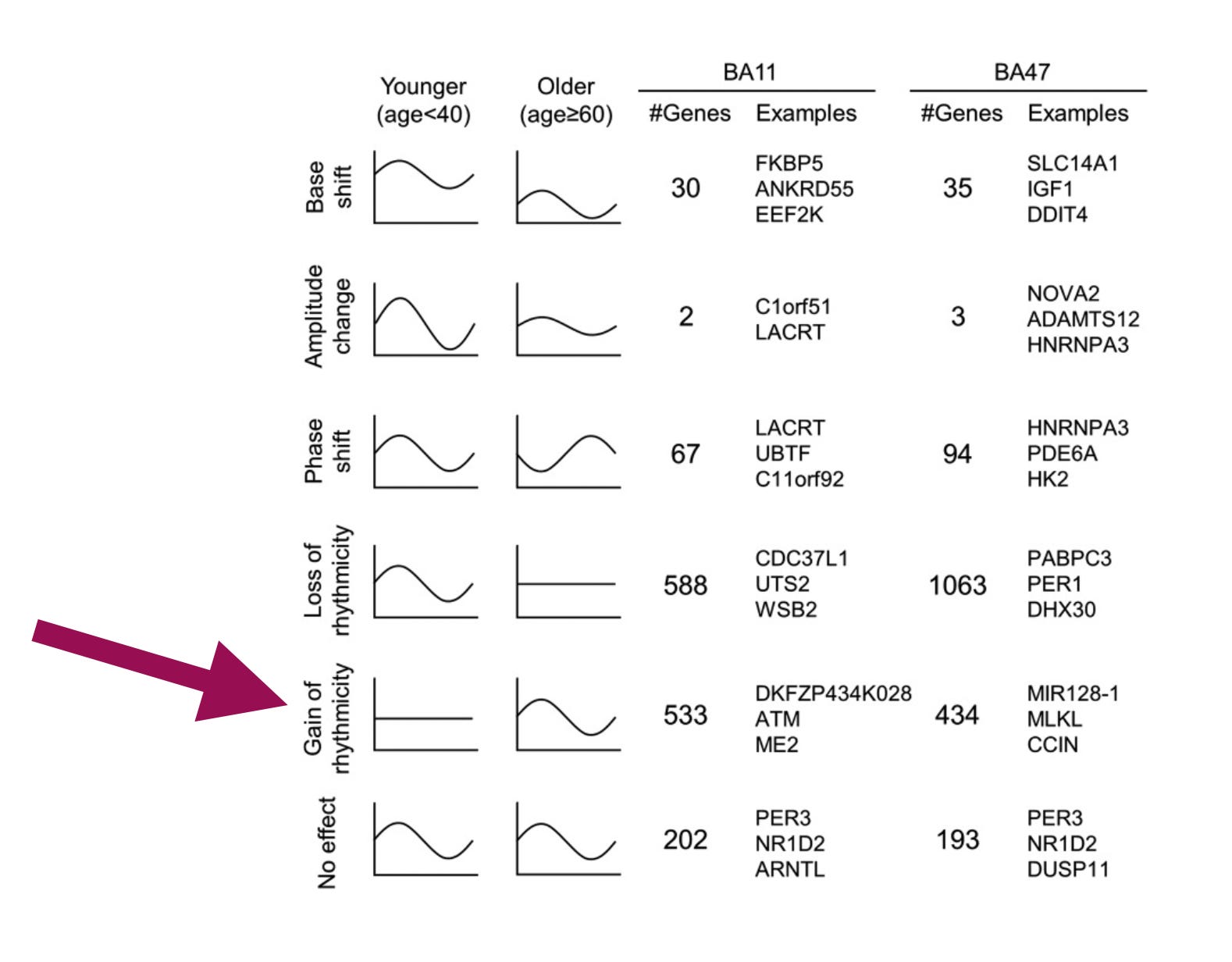
Surely the appearance of so many new rhythms during old age—a period of life characterized by worsening health outcomes—implies circadian amplitude suppression is a woefully inadequate way of describing what’s going on! Checkmate, etc., etc.
Ah, but remember: the claim is that the presence of a circadian problem implies the presence of a low amplitude somewhere, not “every rhythm in every circadian problem is squished.”
Here, I’m going to draw on my own life. Consider the rhythm of my toddler breaking stuff daily in my home. Generally, this is a low amplitude rhythm: he breaks nothing at night while he’s asleep and maybe 0.5 things per week during the daytime hours. Averaged over many days, it would look like a very flat rhythm with some elevation during the times he’s awake and a flat zero (0 broken things per hour) from 7 pm to 7 am.
But this is only because his ability to break things is constrained by my high amplitude inhibition rhythm, where I am actively trying to prevent him from breaking things during the hours I’m awake. If that rhythm gets knocked out—I get sick or distracted by writing a 3,000-word blog post about circadian amplitude—my inhibition decreases, and the amplitude of his destructo-rhythm increases.
Except instead of a toddler breaking things, it’s cortisol, and instead of me, it’s SCN inputs to the HPA system growing weaker. You see where I’m going with this.
How we, in modern life, continually suppress circadian amplitude through our choices and behaviors.
Amplitude suppression might occur acutely. If you typically turn off the lights at 10:00 pm, and I break into your house and turn them all on max brightness at 11:00 pm, your melatonin levels, which have probably been rising for the last three hours, will go down. This is very straightforward, as melatonin is inhibited by light. It’s the night hormone. Light means not night.
Amplitude reduction might also be a state you’ve been driven to, either by disease (e.g., Alzheimer’s), diet (e.g., high-fat), or a long history of confusing inputs to your body (shift work). A person in a more persistent state of low amplitude doesn’t need to be in the light for their melatonin amplitude to be suppressed. Remember earlier, when I said the amplitude of melatonin is best understood relatively, since some people are naturally high producers and that makes it so we can’t use the same scale for everybody? That’s still true. But it’s undeniable that shift workers as a class tend to have lower, blunted rhythms than non-shift workers. Take this person, for example:
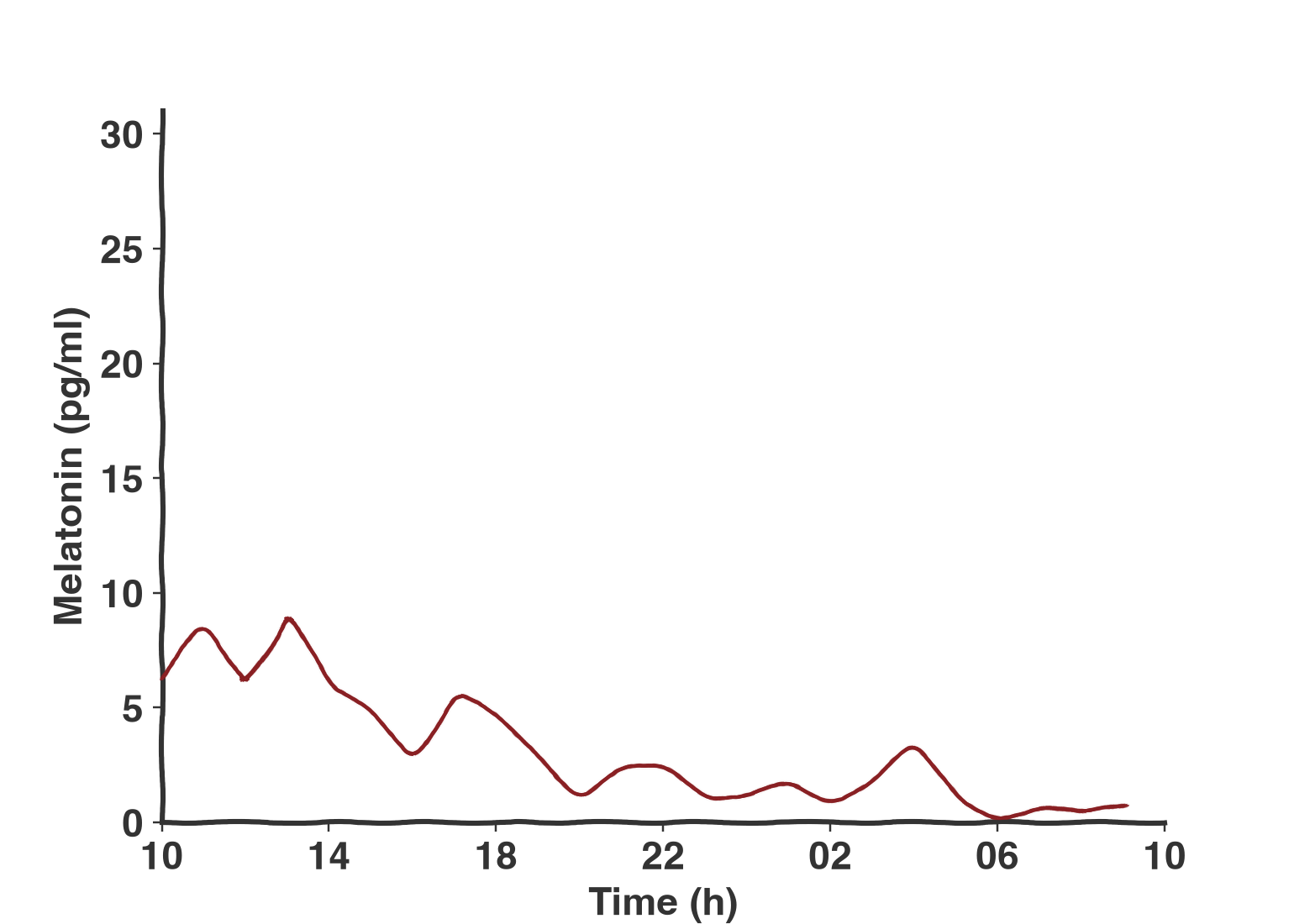
This is real data from a shift working person who was in the dark the whole time as data was being collected. This is a person who should have had melatonin start to clearly rise and fall at some point in the 24 hours they were assessed. Instead, it’s a 24-hour slump to zero. The endpoints on the far left and right, which meet up in rhythmic data, are nowhere near each other. They’re arrhythmic! They’re low amplitude.
But I’m not a shift worker!
But you are a person living in a place with internet in 2026. Which means you’re probably not getting light and dark as regularly as a person who lives by the sun and firelight alone. And you’re almost certainly not getting as bright a bright or as dark a dark as them.
You know what it’s like to be in a groove on a swing on a playground. You’ve got clear momentum. It feels good. If you started bucking your legs wildly back and forth at random times, this would not help you swing higher. Even if you’re not totally random, anything other than resonance with the tempo of the swing will dampen your swing. You’ll be in less of a groove; you’ll have lower amplitude.
The leg bucking here is the stand-in for the clock inputs (light, activity, wakefulness, sleep) that you want to do rhythmically, in sync with the twenty-four-hour day. Most of us aren’t all that rhythmic. Modern life has conditioned us that sleep duration is what we should care about (8 hours a night) without much attention paid to when those eight hours happen. Yet it turns out that sleep regularity is a better predictor of mortality than sleep duration. Why? Surprising no one, I say amplitude suppression caused by irregularity of inputs to the body’s clock (see Figure 2 in here for a visual). You’re lower amplitude, so you get less of the things you want—say, tumor suppression—when you want them, and more of the things you don’t want—say, inflammation—when you don’t.
{kind=link}
And it’s not just the inputs being irregular that keep us out of a circadian groove. We get way less light during the day and way more at night, the equivalent of wimpily flopping our legs forward and back on the swing in place of good, strong kicks. And we make lifestyle choices, like high-fat diets, that impair our ability to groove at all, the equivalent of trying to swing in big honking clown shoes that scrape the dirt on each back-and-forth.
Hear, as I’m talking to you, the beep-beep-beep of a heart monitor in your medical drama of choice. When the regularity of those beeps starts to break down, it’s a sign that the big flat is coming; the lowest amplitude of them all. This is what we’re doing to ourselves when we keep the lights on late and eat at 11:00 pm. We are all low amplitude.
You’re healthy because you’re flat?
Of course, no biological story is ever just that simple. When you knock out the circadian clock, mice die significantly sooner than they otherwise would. There are some knockout mouse lines where they’re more vulnerable to certain cancers. Yet there are some knockout mouse lines where they’re less vulnerable to certain cancers. What gives?
When you lose amplitude, you lock in at some value—the MESOR of your dampened oscillations. Low amplitude, I claim, is bad because you have either too little of something at some time, too much of something at some other time, or some combination of both. But there’s no reason why you couldn’t also, as part of being low amplitude, lock something in at a level that’s both higher than it should be and actively beneficial in some contexts. Imagine you flatten your rhythms in a way that happens to make your baseline DNA repair higher, for instance. You’ll still die earlier from lack of clock, but you won’t die of cancer.
I’m sticking this here at the end because biology is a great humbler. I could come out and say “High amplitude for all! Brighten the ICUs!” and then it could turn out that it’s actually good to be low amplitude when you’re very ill in order to keep things from swinging too low at any point. I could tell cancer patients to make their rhythms higher amplitude, and it could end up boosting the vitality of both tumor cells and healthy cells alike. With anything health and biology related, blog posts are just about the only place you can be carefree and silly. Actually translating to patient care means taking careful steps and being obsessively paranoid of the potential pitfalls at every turn.
But at the very least we should be taking those steps in the right direction. And the right direction is towards reframing much of chronic disease as a form of circadian death.
So what do we need?
We need a good, easy way to measure amplitude. We need something that, with a single sample or lightweight tracking, can give you a quantitative assessment for whether someone’s flat or not. There are better ways of using activity to get an estimate of amplitude than just “how much motion did you do,” and blood and hair tests of gene expression are ripe with potential. More work on these is critical. We can’t communicate about amplitude if we don’t get very precise about what we mean, and shared measurements are the first step towards getting there.
We should make sure people know the recipe for high amplitude by heart: bright days, dark nights, same time every day. Same principle for food. Don’t eat at times when your body doesn’t expect it. Avoid things that can trigger low amplitude by clogging up the clockwork of your body’s machinery, like high-fat diets.
And we should probably stop saying “circadian misalignment” if we want people to really, actually care about circadian rhythms. Misalignment sounds like something an orthodontist could fix. Cosmetic, temporary; “the frame was misaligned on the wall so I aligned it.”
People out there are starving their system of DNA repair at night and deluged by inflammation during the day. They’re glutting their microglia with cholesterol beyond what the daily flush can clear, and frying their SCN with light at its most vulnerable hours. There should be an urgency to rescuing dying circadian rhythms, not a shrug. Circadian amplitude is whole-body health. Let us not go gentle into that long flat.
Thanks to Marc Ruben for comments and feedback on this post!