

Thoughts on the retracted Nature Medicine immunotherapy paper
Can a long half-life drug have a time-of-day effect?

My new neighbor knocks on my door at 7:00 pm. “Hi,” he says. “Just wanted to introduce myself. Hope I didn’t interrupt your evening.”
“What a nice young man,” I say as I shut the door behind him five minutes later. “I’ll remember him fondly.”
(Jump one universe to the left).
My new neighbor knocks on my door at 12:00 am. “Hi,” he says. “Just wanted to introduce myself. Hope I didn’t interrupt your evening.”
“What a freak,” I say as I shut the door behind him thirty seconds later. “Who does that? Who introduces themselves for the first time at [expletive] midnight?”
The same event—meeting the same neighbor—hits five hours apart in two identical universes. In one, our relationship starts congenially. In the other, he’s forever memorialized in my brain as Weird Guy (Do Not Interact).
The question posed today isn’t whether I’m right to respond this way (of course I am) or if my estimate of 9:00 pm as the time when appropriate-to-stop-by becomes don’t-do-it is correct (yes).
The question is whether or not this happens with immunotherapy for cancer.
An extremely fast primer to get everyone up to speed
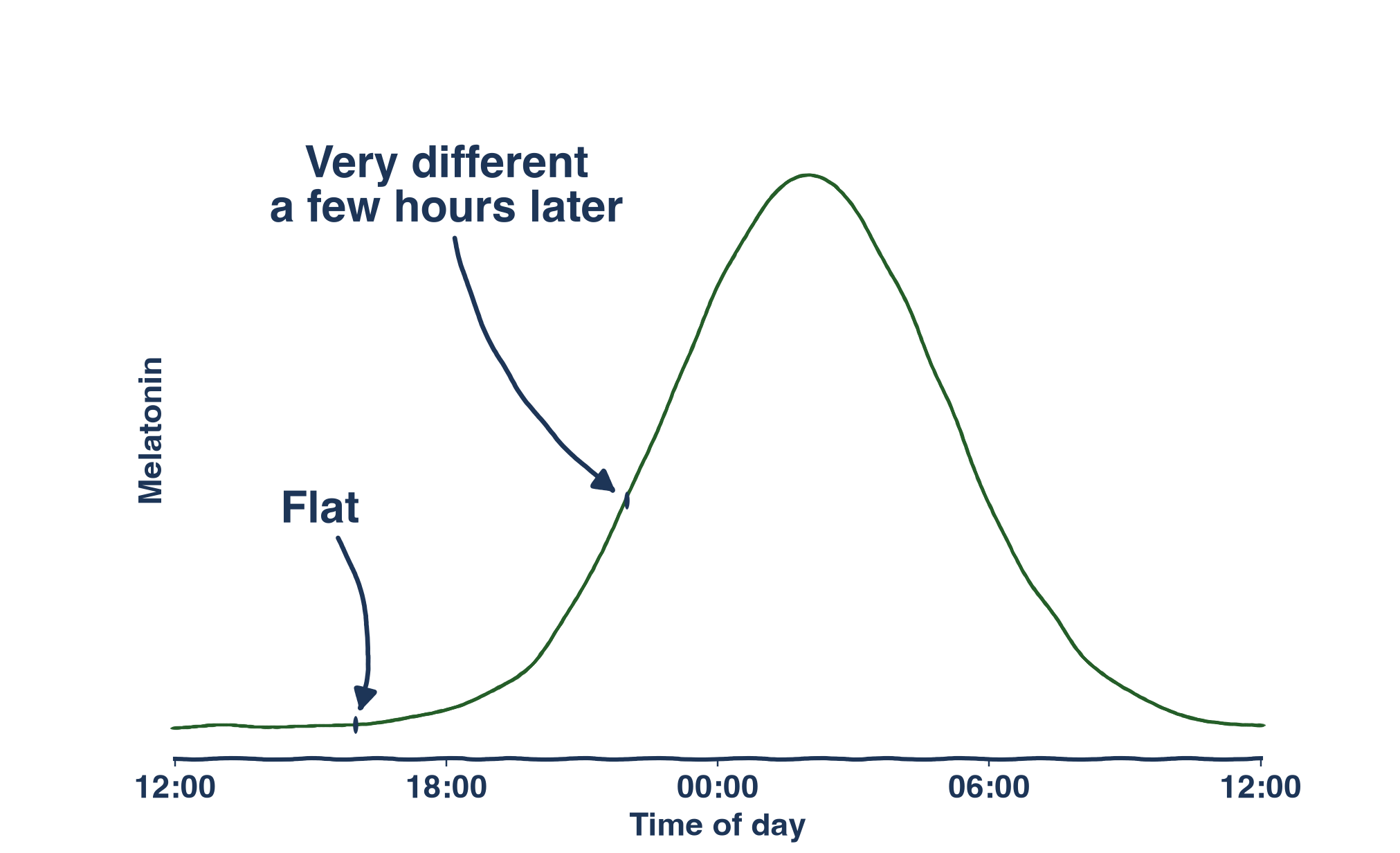
Taking drugs at different times can make them better or worse at their jobs. We know this for sleep drugs. Nobody takes Ambien at 7:00 am to help them sleep better that night. Take melatonin in the evening and it will speed up your body clock, shifting your rhythms and making you feel sleepy earlier. Take it in the morning, and it will have the opposite effect.
But sleep is not the only circadian rhythm, just the most visible one. Plenty of other things in your body have rhythms you’re at best dimly aware of. I only notice rhythms in grip strength when I’m trying to open a jar at 6:00 am in the morning, and I only notice rhythms in immune response when my sinus infection symptoms get abruptly worse at night. Me noticing these things is not a precondition to them mattering, though, and it stands to reason that plenty of non-sleep drugs should have a “best time” of administration.
…if they have a short half-life.
Short half-life means they get in and out of your body quickly enough for timing to matter. Caffeine has a short half-life, which is why I can drink cold brew in the morning and have it cleared out of my system in time for bed sixteen hours later. Hypothetical 20-day half-life caffeine would be a terrible idea—it would mean that the amount of caffeine in my system would take 20 days to fall to half its initial level. If my first sip of long-acting coffee happened at 6:00 am, then 98.28% of my dose would still be floating around my body 12 hours later at 6:00 pm. Who cares that I drank it in the morning? I’m consigned to weeks and weeks of bad sleep either way.
It’s simply very, very clear: if something’s going to have a time-of-day effect, it better not have a 20-day half-life.
Hmm.
Except immunotherapy for cancer kind of seems like it might?? Or rather: Over and over again, retrospective studies have found time-of-administration effects, with morning dosing being better than afternoon dosing. This is weird, and from just about the first moment retrospective results dropped, people have been calling it out as weird.
After all, the immunotherapy drugs in question have VERY long half lives (22-25 days). Everything in my long half-life caffeine example applies to them. The amount of drug in your system 12 hours after an initial dose is essentially identical to that initial dose. How could timing the dose possibly matter when the difference it makes is on the order of 1%?
A lot of people have spent a lot of time thinking about this and have arrived at the same conclusion: it has to be a first exposure thing. If it’s real, it has to be something like what’s going on with my neighbor. The half-life of my neighbor, after all, is maybe something like 40 years1. The same amount of my neighbor is on my street every day of the week for as long as we both live there. But a five hour difference in time-of-first-introduction is all it took for me to permanently remember him as “fine” or “freak.”
But is something like that actually what’s going on?
The case for No
Not every retrospective study finds a morning benefit to immunotherapy for cancer.
Many do, see: [Karaboué et al., 2022], [Catozzi et al., 2024], [Qian et al., 2021], [Gonçalves et al., 2023], [Patel et al., 2024], [Nomura et al., 2023], among others (17 covered in [Karaboué et al., 2024] alone).
But not all of them do, see: [van Rensburg et al., 2022], [Janopaul-Naylor et al., 2024].
So if this is a phenomenon that only appears sometimes, it is natural to trust it less than if every study reported a positive result. It’s not “being struck by lightning is bad for you” levels of clear-cut causality. And speaking of casualty,
There are non-circadian things that could drive a time-of-day effect.
This one is extremely compelling! Whenever I’ve been pregnant, I’ve done everything in my power to schedule appointments as early in the day as possible because I’ve got other stuff to do later in the day, and I don’t want that stuff to be interrupted. I’m an early bird, and earlier is just easier for me.
Early birds tend to be healthier than night owls, and it seems completely plausible that early bird patients could be both healthier and choosing to come in earlier.
Or better yet: I’m less likely to schedule an infusion for 8:00 am if I live far away from the hospital. If I live far away, I’m more likely to live in a rural area, which correlates with worse health and fewer resources. So people who are more likely to be doing worse are systematically scheduled to be later in the day. That’s all you’d need for an effect like this to arise!
This is the argument of a paper from this week where the authors include “distance to the treating institution” in their statistical model and find no relationship between timing and survival (while also finding that the farther you live, the less likely you are to have an early appointment).
The natural way to address these confounders is with a randomized controlled trial (RCT), where the study team, not the patient, picks when they get their infusion. But, unfortunately,
The one prospective randomized controlled trial just got retracted.
Adam Rochussen of the Salk Institute has a really great write up on this, so go read that first. Briefly:
Mid-trial updates to the clinical trial record
Protocol submitted to the journal with the wrong date
Fewer dropouts than expected (interestingly, also flagged in another questioned chronomedicine study)
Kaplan-Meier curves looked less stair-steppy than expected given the typical scan schedule
And perhaps most eyebrow-raising of all, the effect size was enormous. Which is surprising because
A very large morning-to-afternoon swing would be weird.
Big swings in circadian rhythms can happen, of course. Melatonin goes from nothing to ON over the course of a few hours.
But a big morning-to-afternoon swing implies that a hypothetical efficacy curve looks either like this:
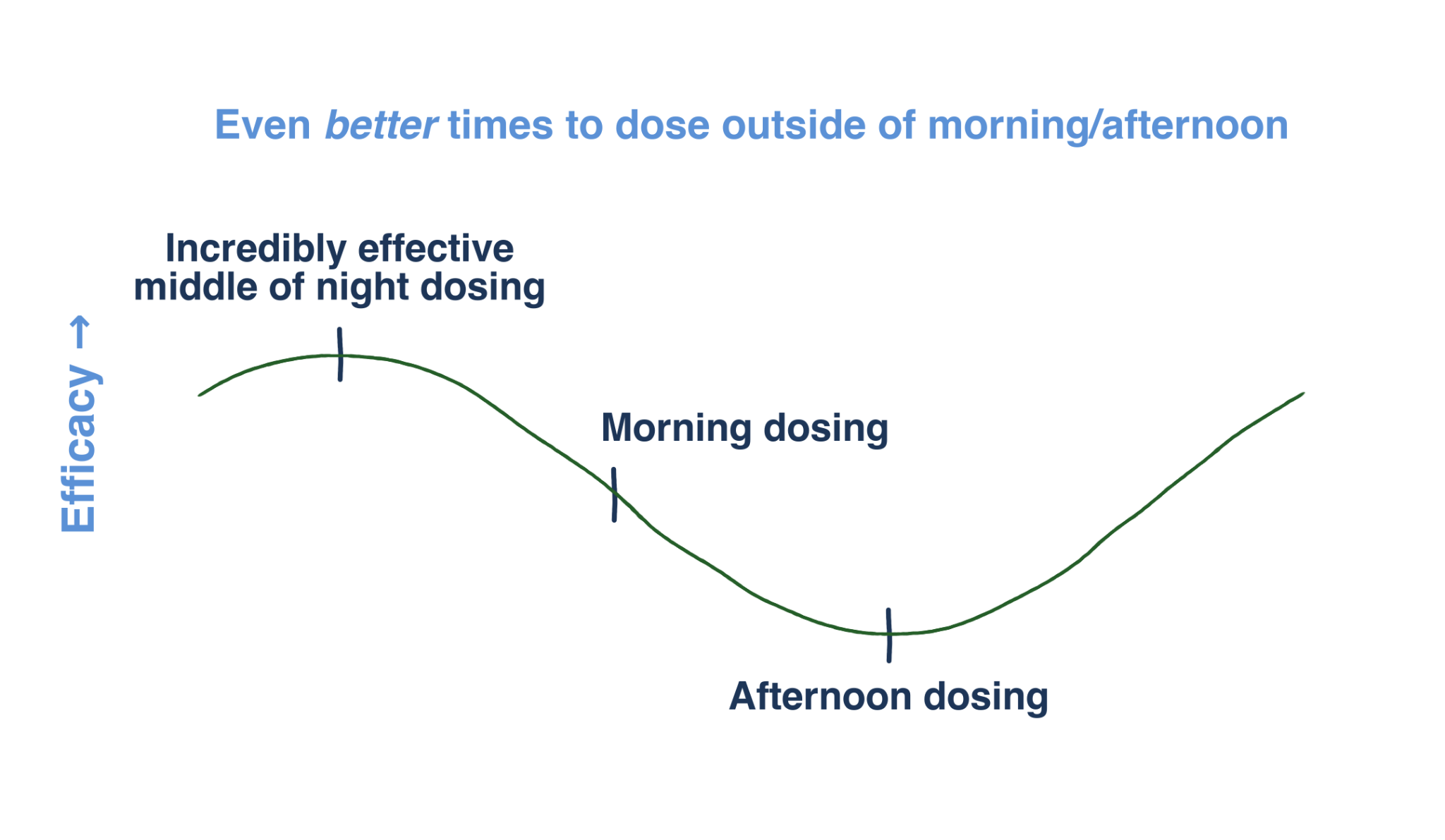
Or this:
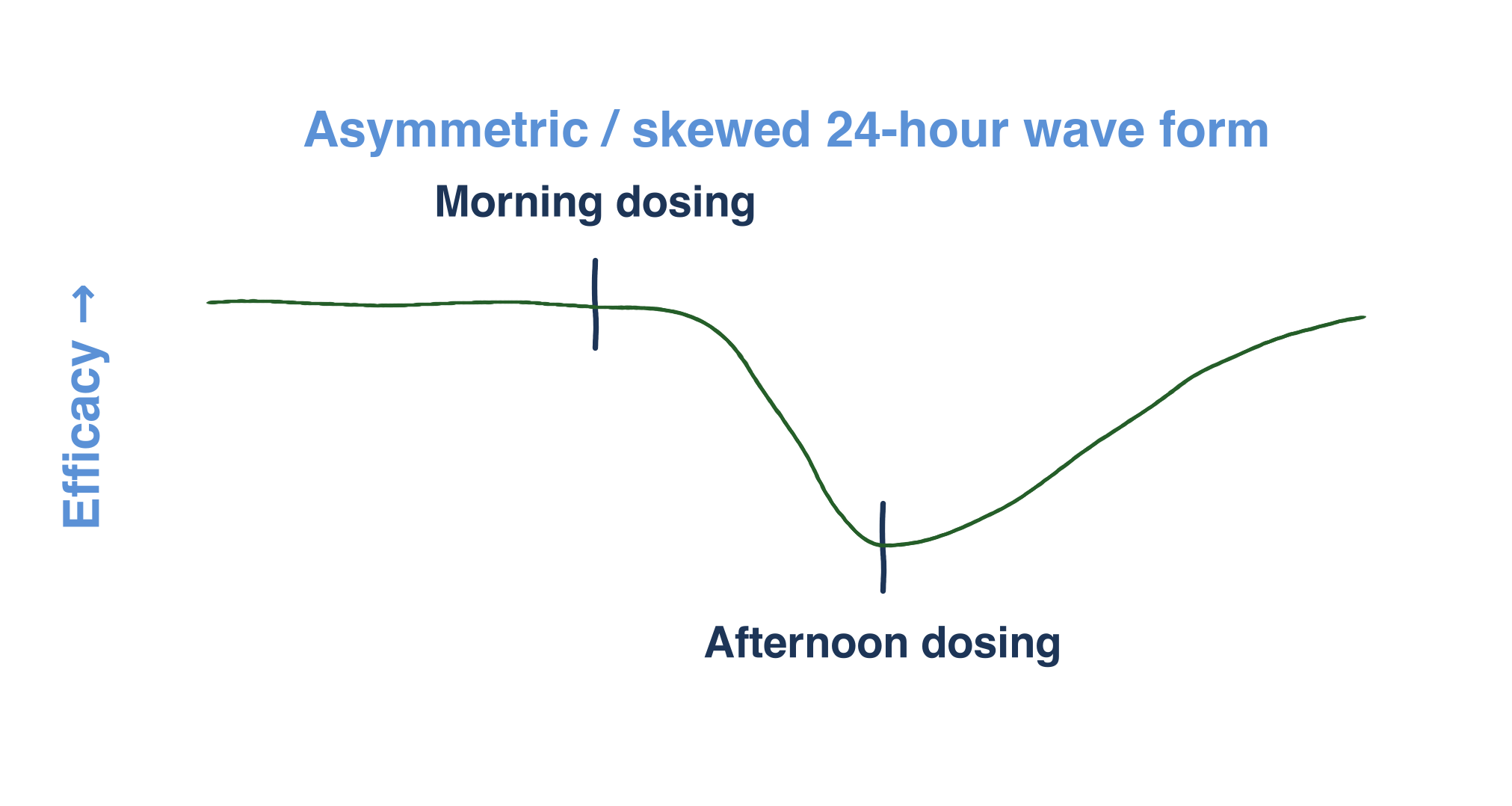
Given that nobody’s reported that extreme night owls getting infusions in the morning (i.e., their biological night) go into complete remission right away, I’m doubtful that that the first one is what’s going on, and suspicious of the second one as a hypothetical and sharply skewed circadian rhythm without any clear mechanism behind it.
But I’m four pages into this blog post, and I’ve mostly just remade arguments people made before the immunotherapy RCT was retracted. So in the interest of adding something new, let me now make
The case for “well, hang on”
Not every retrospective study finds a morning benefit
Let’s assume there IS a real circadian time-of-day effect to immunotherapy for cancer. What could we expect—knowing nothing about what’s played out in the last six years—to happen?
Well, for starters, wall clock time (AM vs PM) is not biological. Within individuals living in the same time zone, you can get a ~10-hour spread of biological times at the same wall clock time2. Biological time is set by the history of synchronizing signals a person gets (food, light, activity) which can be wildly different between people living in the same home, let alone hospital service area.
This means you’ll have some people coming in for an afternoon appointment during their body’s biological morning or a morning appointment during their body’s biological afternoon. The spread in biological time will blunt the observed effect size. Or, in graph form:
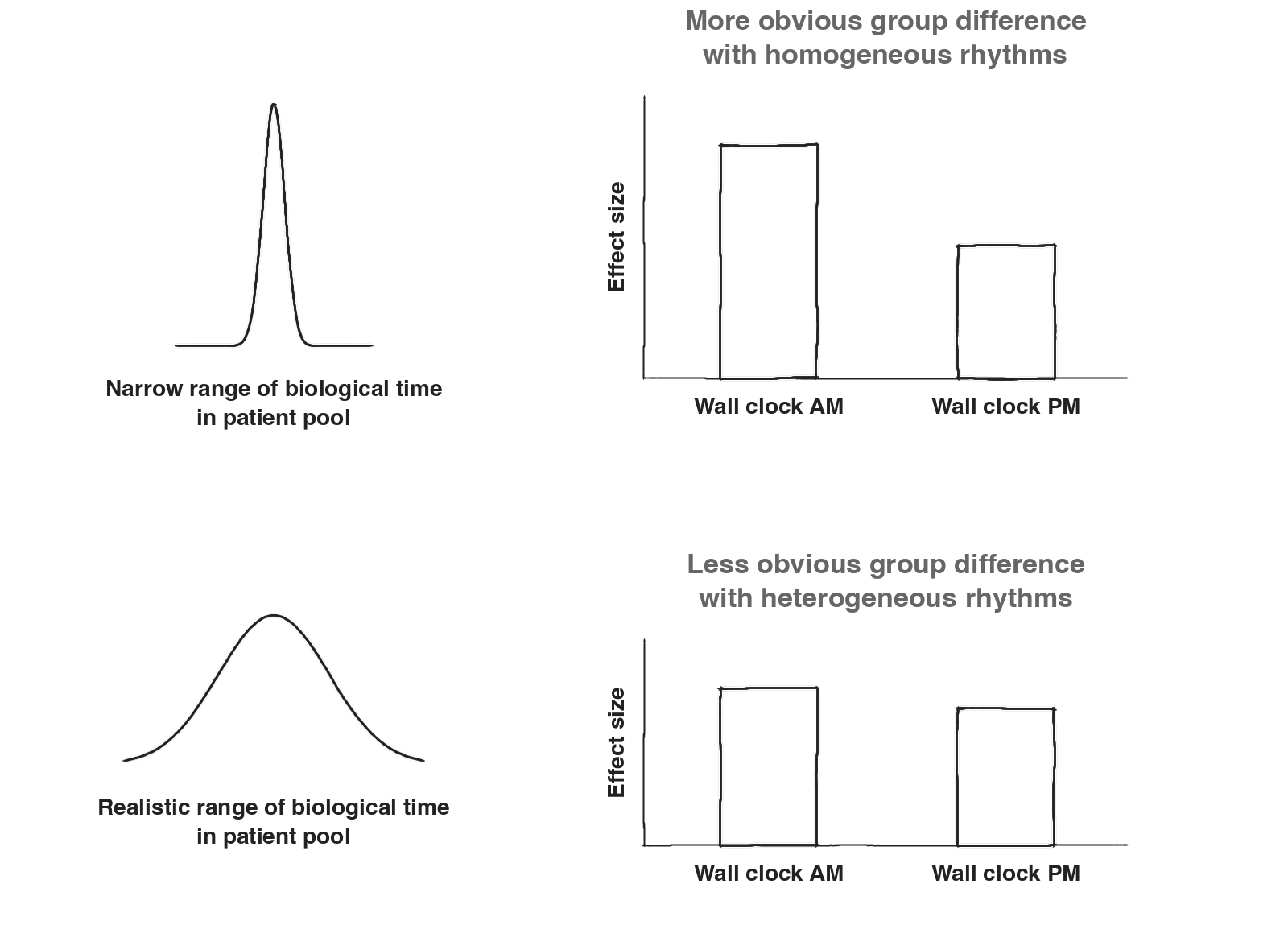
Participants can also have flatter or more pronounced rhythms (circadian amplitude), which could similarly blunt or enhance a real effect.
Plus the authors in these retrospective studies are all using different definitions of “morning” and “afternoon” and different ways of deciding which infusions to use in their analysis (all of them, first one only, first few, etc.), making direct comparison a challenge.
Finally, if there’s one lesson I’ve learned from reading the cancer literature, it’s that all tumors act the same way and that if something is true for one of them, it’s true for all of them. (I pull a baseball bat out from behind the desk.) No! Of course not!
So to “not every retrospective study finds a morning benefit,” I’d say “yeah, as expected”.
There are non-circadian things that could drive a time-of-day effect.
Sure, but there’s preclinical data showing that the timing of the first dose (of two) can dominate tumor response ([Wang et al., 2024], Figure 5E):
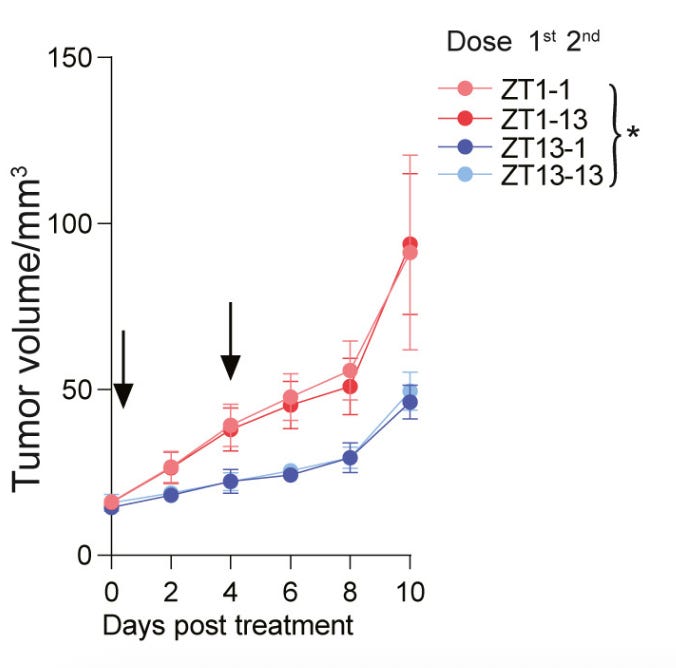
In the above, the red lines show what happens to tumor growth in mice when the first of two doses is given at the start of the rest period, while the blue lines show what happens when the first dose happens at the start of the active period. Regardless of when the second dose happens, the first dose drives the effect. A very valid response to “what if it’s all people who drive long distances to the hospital being sicker?” could be to say “trust us, that’s not happening in mice.”
But I want to engage more with “distance from hospital site” as a possible explanation for observed time-of-day effects, both because mice aren’t people, and it’s a very reasonable explanation to propose. The thing about it that gets me is this: People come to the hospital for a lot more than just immunotherapy. If it really is just rural, far-away people being more likely to be worse-off, shouldn’t we see a morning benefit for lots of other things as well…? Chemotherapy, appointments in general3— why not morning superiority in all those cases? Why only immunotherapy?
You might say “well, maybe we DO see that morning is best for all of those,” but I’ve looked at infusion times for chemotherapy in fairly large datasets and seen no time-of-day effect4. With so much historical data out there, I’d expect that other people have done the same. Why aren’t there a slew of papers showing equally huge benefits to morning for all the many things people drive to the hospital for that aren’t immunotherapy?
Once again, we need a prospective RCT. And, of course,
The one prospective randomized controlled trial just got retracted.
Yep, but “this study is not reliable” does not mean “this phenomenon is disproven.”
Lotta people out here mistaking If P Then Q for If Not P Then Not Q. That’s not how it works.
The contrapositive of “if there’s a randomized controlled trial supporting the timing hypothesis, then it’s likely a real effect” is “if it’s not likely a real effect, then there isn’t a randomized controlled trial supporting the timing hypothesis.” Not “no trial, no effect.”
You could say that if there had been a real effect in the retracted study, then the authors wouldn’t have needed to change the trial registration/protocol, etc. But about all of this, there’s a lot we don’t know. I’m more inclined to assume unfortunate sloppiness than malfeasance until I’ve got a blindingly obvious reason to believe otherwise.
And, finally:
A very large morning-to-afternoon swing would be weird.
But hey, weirder things have happened.
Final thoughts
Is immunotherapy in humans like my neighbor example, where a few hours difference in time-of-first-introduction for something with a long half-life has a huge impact on the response to that thing forever after?
My guess in this moment is: ehh.5
Not because of any certainty I have that such a thing is biologically impossible (the mouse data in [Wang et al., 2024] is this, after all), but because it’s just not a slam dunk in the human data. Consider [Fletcher et al., 2025], where late immunotherapy shows up as bad for you when you use all the infusions in your calculations, but not when you use only the first four. This is the opposite of [Nomura et al., 2023], where they find a much clearer signal from the first infusions, but it’s enough to make me look askance at the “first infusion is the only thing that matters” hypothesis.
I’ve sometimes wondered why more people haven’t put out a compounding argument, and I’ve usually landed on “because it’s so simple it’s embarrassing, and people will say `that’s not how cancer works, idiot’.” But I, fearless, will make the argument anyway: Let’s say you get one dose in the morning, and it reduces your tumor to 98% of the size it would have been with afternoon dosing, a near negligible difference. Then, weeks later, you do it again and again, always in the morning, always getting that 2% edge. Eighteen sessions later, 0.9818 = 0.695—a thirty percent improvement over the always-afternoon dosing regimen! Let’s say it’s a 1% edge instead: 0.9918 = 0.835. Still pretty good!
Yes, most people won’t be all-morning or all-afternoon, and plenty of people don’t get to 18 sessions, so you’d expect the effect size to be smaller in practice. And, yes, for sure, this is a massively simple model. But at least it’s a model I understand, and—best of all—one that can pair nicely with other hypotheses, including a weaker form of the first infusion effect, where first exposure matters but isn’t everything.
Maybe the thing that unifies all the data to-date is some combination of compounding small benefits, a reasonable first infusion effect, and the inherent noise of biological time making clear morning/afternoon cut points unstable. Or maybe it’s all confounders! At the end of the day, it’s still retrospective data. We need an RCT that sticks around.
There are ongoing randomized controlled trials at other sites looking for timing effects right now. They’re surely going to be very careful about protocol updates and providing accurate documents to the journal. They’ll be highly motivated to make sure the characteristics of the different timing groups are as balanced as possible. They might find absolutely nothing when they do this, which will be a glorious vindication for those who questioned the results from the beginning and a textbook example of why RCTs matter.
Or they might, even after controlling for everything they can think of, still find a benefit to morning dosing. If that happens, there will be some people who nonetheless doubt the result. Some because timing medicine sounds like astrology to them, some because debunking is objectively fun, and some because it would be a massive pain in the ass to have to change clinic times. I’m sympathetic to all of these, minus the “timing medicine is astrology” take. Chronobiology grad students did not stay up all night in the lab sampling every two hours to be disrespected like this. They stayed up to be disrespected for being grad students.
References
Catozzi, S. et al. (2024) ‘Early morning immune checkpoint blockade and overall survival of patients with metastatic cancer: An In-depth chronotherapeutic study’, European journal of cancer (Oxford, England : 1990), 199. Available at: https://doi.org/10.1016/j.ejca.2024.113571.
Fletcher, K. et al. (2025) ‘Immune checkpoint inhibitor infusion times and clinical outcomes in patients with melanoma’, The oncologist, 30(1). Available at: https://doi.org/10.1093/oncolo/oyae197.
Gonçalves, L. et al. (2023) ‘Immunotherapy around the Clock: Impact of Infusion Timing on Stage IV Melanoma Outcomes’, Cells, 12(16). Available at: https://doi.org/10.3390/cells12162068.
Huang, Z. et al. (2026) ‘RETRACTED ARTICLE: Time-of-day immunochemotherapy in non-small cell lung cancer: a randomized phase 3 trial’, Nature Medicine, 32(4), pp. 1233–1240.
Janopaul-Naylor, J.R. et al. (2024) ‘Effect of time-of-day nivolumab and stereotactic body radiotherapy in metastatic head and neck squamous cell carcinoma: A secondary analysis of a prospective randomized trial’, Head & neck, 46(9), pp. 2292–2300.
Karaboué, A. et al. (2022) ‘Time-Dependent Efficacy of Checkpoint Inhibitor Nivolumab: Results from a Pilot Study in Patients with Metastatic Non-Small-Cell Lung Cancer’, Cancers, 14(4). Available at: https://doi.org/10.3390/cancers14040896.
Karaboué, A. et al. (2024) ‘Why does circadian timing of administration matter for immune checkpoint inhibitors’ efficacy?’, British journal of cancer, 131(5), pp. 783–796.
Nomura, M. et al. (2023) ‘Timing of the infusion of nivolumab for patients with recurrent or metastatic squamous cell carcinoma of the esophagus influences its efficacy’, Esophagus : official journal of the Japan Esophageal Society, 20(4), pp. 722–731.
Othus, M. et al. (2026) ‘Addressing Biases in Analysis of Time of Infusion: NCI/SWOG Trial S1404 Among Participants With High-Risk Resectable Melanoma Who Received Adjuvant Anti-PD-1 Therapy’, JCO oncology practice, p. OP2501413.
Patel, J.S. et al. (2024) ‘Impact of immunotherapy time-of-day infusion on survival and immunologic correlates in patients with metastatic renal cell carcinoma: a multicenter cohort analysis’, Journal for immunotherapy of cancer, 12(3). Available at: https://doi.org/10.1136/jitc-2023-008011.
Qian, D.C. et al. (2021) ‘Effect of immunotherapy time-of-day infusion on overall survival among patients with advanced melanoma in the USA (MEMOIR): a propensity score-matched analysis of a single-centre, longitudinal study’, The Lancet. Oncology, 22(12), pp. 1777–1786.
van Rensburg, H.J.J. et al. (2022) ‘The effect of circadian rhythm on clinical outcome in patients receiving pembrolizumab in the INSPIRE pan-cancer trial’, Journal of Clinical Oncology [Preprint]. Available at: https://doi.org/10.1200/JCO.2022.40.16_suppl.2589.
Wang, C. et al. (2024) ‘Circadian tumor infiltration and function of CD8 T cells dictate immunotherapy efficacy’, Cell, 187(11), pp. 2690–2702.e17.
With thanks to Adam Rochussen, Eric Canton, Doug Marttila and Franco Tavella for thoughts on this blog!
joking, mostly
even bigger for shift workers
doctor performance, notwithstanding—I understand that doctors being more alert in the morning could yield better outcomes for appointments, but I don’t see a strong role for doctor alertness for a pre-scheduled infusion time.
paper in the works
I’m “ehh”-ing immunotherapy time-of-day effects being driven by first infusion time here!! Not chronomedicine! Still very bullish on chronomedicine!!
The senior author for Wang et al., Cell 2024, is also a corresponding author on the retracted Nature Medicine paper. There is a small group of investigators who have pushed this theory very hard and are very invested in it - apparently at the cost of honest science.